It's really quite perverse, living with chronic pain and having profound memory issues. On the bad days, it often feels like it hasn't been quite this bad in a while (even if yesterday was actually quite awful), and on the good days, you begin to doubt that it was ever really all that bad, save for a few memorable incidents. It really screws around with your self image, because you never quite feel like you can trust either your own opinions or memories.
Since I've been working with the VA to control things, I've tried to be more faithful in recording changes and statuses regularly, but it's hard to figure out exactly what to say, and when. There's little objective value in just repeating "it really, really hurts, and makes me want to vomit", so I'm afraid that many of my entries tend to be needlessly specific and clinical, even if no one else will ever see them. Even so, it's easier for me to believe myself when I can more clearly see the trends and spikes in depression and pain. That helps, some, but doesn't hold for long. It's really, really messed up to be in the middle of a horrible attack and still feel like you might be a hypochondriac.
I'm a little conflicted right now, too, about the concern the family is showing for me. It's gotten so that nearly any time I'm in pain or look uncomfortable (she often sees me holding my head or cringing from light long before I'm consciously aware of anything more than discomfort), Eden will immediately ask me "Do you need me to take you to the ER?"
It's the right question to ask; I know she only wants to help and in turn feels the same incredibly intense need to fix things that I do when she's in pain, but at the same time, it makes me feel terribly odd, every time. On the one hand, the VA isn't really set up to do anything but send you to the ER if you don't already have an appropriate appointment, and on the other, I sure as hell don't want to crowd the only VA emergency room in the Portland area when they routinely only have 2 doctors on duty at once. So, again, I tell her "No, it's just a bad day.", which has absolutely been the truth recently, but the bad days have been coasting along at just below crisis level.
On the plus side, I'm still getting the occasional block of daylight hours that ends up relatively symptom-free, even if the mornings and evenings aren't doing so hot. The nausea had even been staying away entirely for a few days in a row last week, so Eden, Cassie, and I hopped in the car on Friday and went up to Home Valley to swim, just past Stevenson, WA. It was actually my first run there in months, even though the girls have been heading there regularly all summer, as their respective tans attest. The length of the trip and the associated twists and turns just made it an impossibility while my stomach was even slightly twitchy, as our few aborted group attempts prior will attest.
In this case, however, we actually had a wonderful time, something of an appropriate goodbye to the season on the autumnal equinox, and we even got to go by Granma's Gedunk and get a scoop of ice cream before they closed for the year. The heat in the air was much less oppressive there, and it was still pretty warm in the water (I tend to get a bit shy about just jumping in when it's icey.) My head even held long enough for me to take over driving on the way home, as Eden was just bushed.
Yesterday morning was pretty good as well; I got to accompany Eden out to see Vivian and do some housework for her, as has become a bi-Monday habit. Again, restrictions in movement ability have kept me from doing this for months, and I missed seeing her outside of the occasional family group meal. Very odd day, symptomatically, actually - much of the day was simply swept aside by massive waves of dizziness and nausea, fortunately waiting to start until we were already out for sushi with her. I absolutely love pickled ginger on sushi rolls, and it helped my stomach quite a bit for the short term.
Once we got home, we got something of an explanation for the big charge, if not a reason for it. Upon checking,my blood pressure was 30-40 below my average, starting at 57/99 at 73 bpm, and holding in that range for nearly the entire day. Normally, I run very high, staying in the 110-120/150-160 at 100+ bpm, with spikes over the 160 line (official hypertension) when I'm in active pain. Climbed back towards my normal range today, but still feeling pretty off.
It's far to early to make any definitive statements, but all the same, it feels like the new magnesium oxide and gabapentin combo that's supposed to help level out my symptoms over the long term is having some effect - at the least, my answers about the ER hasn't had to be "YES!" since I started taking it almost two weeks ago, and I'm still not quite up to the final level of dosage yet. If only I could get an answer on increasing my number of pills for my rescue meds that I'm supposed to take at the onset of an attack to blunt it (currently I'm allotted 9 pills per month... and I'm having migraines twice a day, most days), I'd actually be pretty happy with the progress over the short term. At the least, when I actually do break down and use one of the rescue meds, it does seem to help noticably, and usually within an hour or so (my last usually took about 2.5 hours to do anything, if they were going to).
We'll see how things turn out. I did receive my results back from the IGE allergen test, and if I'm interpretting the number correctly, I'm not significantly allergic to anything they test for. (Again the double-edged sword - I don't have to give up any major food group for life, but no instant fix from it either).
This Friday is actually going to be rather interesting, or at least I think so. I'm going in for a trans-esophageal echo-cardiogram (an ultrasound probe down my throat, so as to be able to get right up next to my heart and get a very clear picture of the structures.) They'll be looking specifically for a malady known as PFO, or Patient Foramen Ovale. Here's the theory on what it is and why it sounds like a perfect match, to me: When you're in the womb, your mom's lungs are doing all of the breahting for both of you, so there's an open passage in your heart that connects the right and left halves, effectively bypassing your own system. Normally, this closes completely before birth, and the halves are completely independent, with one half pumping deoxygenated blood from the body to the lungs, and the other pumping oxygen-rich blood back out.
If I do have PFO, it means that this passage is partially open again, and may be allowing some de-oxygenated blood to bypass the system, which accounts for so many things, in my head. Not only is it potentially directly responsible for the migraines, but also explains the high blood pressure/bpm (more work to do the job if it's a less efficient gas exchange), the extremely volatile and unpredictable nature of my attacks, and the sudden spikes of heart pain (asphyxiation HURTS, thanks to lactic acid build up, and if the cardiac circuit that actually supplies the heart with oxygen gets a spike of oxygen poor blood, that's just what it would feel like. The good news is that if it is PFO, it should be fixable with surgery. This test and possible explanation actually came from one of my former advisors down at Klamath Falls, as he was actually doing a study on this very phenomenon and mentioned that I sounded like an ideal match in my interview. If nothing else, it's a fascinating theory to me, almost beautiful in the elegance with which is would explain so much.
Tuesday, September 27, 2011
Wednesday, September 21, 2011
Steamed
Pissed off and right.... you really, really don't want me in that condition. Unfortunately, that's where I find myself, now. I recently got ahold of the initial results of my compensation and pension exams, and I've got to say, I've very rarely been quite this incensed.
The short version of their findings is: "You don't have any significant issues, and even if you did, we didn't do it." Wrong answer, buddy. The examinations in question were completely screwed up, and in several cases, the examiner simply assumed information that was completely incorrect, in effect falsifying information to provide answers that were more favorable to their side of the table. Seriously not good juju, there.
So, basically, I've been spending the last couple of days working with my local rep and putting together an appropriately scathing and articulate response, and gathering evidence that my issues have been acknowledged as probable effects of the toxin exposure I received in Japan, including some fun internal direction to the C&P department specifically on this subject. If you'd like a better idea of exactly what's going on, I've included the full text of my latest statement below, along with links to the evidence I'm submitting.
Also, as a special "treat" of sorts, I happened across a couple of videos that someone shot of the residential complexes on Atsugi while the incinerator was still in operation. Here they are, if you're curious as to what Jessie and I were living in for a couple of years, especially during the half of the year that winds directed the smog directly to us.
The good news is that my new nurse practicioner seems to be significantly better than my last one, and I've got a number of tests scheduled over the next few months that might help me lock down what's actually wrong a little better.
Joshua ********** – Reference – ********** – File # ********** - Statement in Support of Claim 2
(As dictated to, edited, and organized by Eden **********) September 19, 2011
As my ongoing symptoms of migraine and associated secondary effects have continued to worsen over the past several months, I recently requested a copy of my VA medical health record since March of this year, so that I might provide these reports as additional supporting evidence for my disability claim. Among the reports provided were copies of my Compensation and Pension benefit exams, and I must say that I was dismayed, insulted, and incensed by the opinions given, as well as the manner in which these examinations were given (rushed, incomplete, and in some cases, information/answers assumed by the examiner without bothering to ask relevant questions). Further, I wish to take this opportunity to respond to those opinions and to provide further evidence as appropriate prior to the VA rendering an initial decision on my case, so as to avoid the delay and expense that might be incurred by necessitating an appeal to that decision if it were to be based on these opinions alone.
Firstly, I would like to address a number of discrepancies and note a few items in the two records provided to me. Enclosure #1 is my Navy Medical Record, as provided to me upon discharge. I’d like to note that my separation physical was provided by a pharmacy assistant (as noted on Page 12, 23Oct00), rather than an actual physician, and thus may be considered somewhat suspect in thoroughness. When I left Japan (as noted on page 14, 18Jan00), more frequent colds, sinus congestion, and a pattern of progressively decreasing health were documented already, although my symptoms hadn’t increased to the debilitating level that they have assumed in recent years. Pages 15-19 document that I had been given Health and Environmental Fact Sheet, NAF Atsugi #1 (included as Enclosure #3) as part of the move to on base housing with my first wife, Jessie. I should point out that this move was not optional, and was in fact required as soon as space in on base housing opened up – at no point was an alternative to on base housing made available to service members expressing concern over these environmental issues, and the potential effect of those issues was verbally minimized in every possible way by housing personnel. Additionally, my wife and I were located in building 3056, just over 500 meters from the incinerators in question, and thus had very high exposure to the pollutants throughout our time there.
Pages 10, 13, and 22 document the decrease in hearing acuity that I suffered over my term of service. Pages 13, 23-25, and 75-76 document the skin irritation and psoriasis that developed during this time. Pages 14. and 75-76 document the increased breathing difficulty and bloody nasal discharge over the same period. Conspicuously missing are records of the half dozen or so visits to the doctor that I had documenting intervals of increased blood pressure and dizziness/tingling in the extremities during my service in Japan (the headaches that I currently suffer had not increased to catastrophic level at this time, and thus were attributed to this blood pressure increase). I would like to request that copies of my original medical records from NAF Atsugi and CTF 72 Kami Seya be obtained to provide records of these incidents.
Enclosure #2 is my VA Medical Record, as printed electronically on September 14th, 2011. Pages 44 and 49 both list my habits as drinking rarely; in point of fact I have not drunk alcohol since April of this year, at which point I was asked to discontinue my already infrequent alcohol use so as to avoid additional stress on my system. Pages 24, 64, 67, 70, 73, 76, 79, 83, 86, 88, 91, 94, 97, and 101 all indicate that Topirimate is in current use at the time of respective examinations; this was discontinued on 8/01/11. Page 26 indicates that my mother has dementia and that I had lost 10 lbs; it is my maternal grandmother that had dementia, and I had lost 23 lbs at that point. Page 130 lists ADHD as being symptomatic since childhood; this is incorrect – in fact symptoms have only been present since my military service, and I was not diagnosed as having ADHD until 2006 by Dr. Julien ********** of the Corvallis Clinic in Oregon.
Pages 104-111 are the findings of Dr. Dillon on 8/15/11 for my mental health evaluation for compensation and pension. I disagree with his findings on several specific points. I do, in fact, agree with at least part of his statement on page 105, "...Mr. Byram's depression (including memory gaps) is more likely than not caused by his headaches.", and will in fact state unequivocally that my current depression revolves entirely around my migraines and associated symptoms; I would regard my depression as a secondary symptom of same. As to my memory issues, it is unclear to me how much of that issue is directly related to the headaches and how much is a tertiary symptom created by said depression, or if in fact this is an unrelated symptom created through my toxin exposure at Atsugi.
On page 107, Dr. Dillon selected the response: "Occupational and social impairment with occasional decrease in work efficiency and intermittent periods of inability to perform occupational tasks, although generally functioning satisfactorily, with normal routine, self-care, and conversation." – I would more accurately characterize my situation with this response, found on the same page: "Occupational and social impairment with deficiencies in most areas, such as work, school, family relations, judgment, thinking, and/or mood." He also states that "The veteran's occupational and social impairment is due to his psychological distress/depression." – I disagree with this wholeheartedly. My difficulties with school, work, and social life revolve entirely around my migraines, the inactive time required by them, the difficulty in thinking during an attack, lack of concentration and distraction provided by the severity of the pain and secondary effects, as well as the unpredictability of their pattern. Currently, my symptoms have increased to the point that I have migraines lasting 8-12 hours daily, incurring extreme pain, nausea, dizziness, and provide extreme sensitivity to light and sound as well as visual and spatial distortion. Friends and family have noted an increase in my general irritability, a decrease in logical thinking, and a general depressive mood, typified in the most extreme cases by some level of suicidal ideation during the most severe periods. Onset of symptoms has become both rapid and erratic, causing me to have to forgo driving for myself if at all possible since June of this year.
When I was laid off in 2009, part of the reason that I chose not to return to the workforce and instead attempt to change career fields by going back to school was as a delaying strategy to decrease the level of activity required of me from day to day in response to the increasing severity of my symptoms at that time. I had hoped to find some combination of medicine and/or avoidance of triggering effects that might allow me to decrease the impact of these issues. Instead, symptoms have only worsened since that point, eventually leading to a decision to withdraw from school in June of this year. Eventually, I came to the realization that further time at school at this level of medical control would only serve to increase my debt in terms of school loans without providing significant educational benefit.
On page 109, Dr. Dillon typifies my memory issues as: "Mild memory loss, such as forgetting names, directions, or recent events" – I would argue that the selection of "Impairment of short and long term memory, for example, retention of only highly learned material, forgetting to complete tasks", found on the same page, would be more accurate. At this point, nearly all of my memories of times before the last year or so is missing, and is only able to be mildly prompted by photos and letters from those years. The three years that I had with my first wife, Jessie, are almost entirely gone, and in point of fact, I have great difficulty in even being able to call her to mind. More recent events are, at best, blurry and indistinct, retaining only the most general outlines of experience. Insofar as short term memory is concerned, my daily life has become almost entirely dependent upon electronic alarms and aids, such as writing notes to myself for nearly any issue or concern via my mobile phone, as well as prompting by those around me.
Pages 133-153 are the findings of Dr. Tuna on 6/30/11 for my physical health evaluation for compensation and pension. While I do disagree with several of his findings, and will speak to this further later, the most concerning and immediate issue that I would like to address is that several sections of questions were skipped outright during the interview and simply marked as negative. I would like to address those here. On page 136-138, the sections “Genitourinary ROS” and “Abdominal/Gastrointestinal ROS” were skipped entirely and marked negative.
For Genitourinary ROS, I was not asked if there was a history of abnormal flow, urgency, dysuria, hesitancy, testicular pain, scrotal mass, erectile dysfunction, genital lesions, urethral discharge, flank pain, hematuria, stones, urinary frequency, nocturia, urinary incontinence, dialysis, obstructive voiding, repetitive urinary infection. Accordingly, hesitancy and erectile dysfunction are currently marked as negative and should instead be positive.
For Abdominal/gastrointestinal ROS, I was not asked if there was a history of nausea, vomiting, diarrhea, constipation, indigestion, heartburn, hemmoroids, hernia, abdominal mass, abdominal swelling, regurgitation, jaundice, fecal incontinence, post-prandial symptoms, dysphagia, hematemesis, melena, pancreatitis, gallbladder attacks, abdominal pain. Accordingly, nausea, vomiting, heartburn, gallbladder attacks, and abdominal pain are all currently marked as negative and should instead be positive.
On page 138, under Psychiatric ROS, history of speech difficulty, memory problems, and sleep impairment are all currently marked negative and should be positive. I often experience aphasia during migraine attacks, have extensive memory issues as indicated above, and currently experience both insomnia and night terrors. Both page 144 and 147 indicate that I was currently in school at the time of examination, when in fact I had already stopped going to school. Page 145 indicates no history of dizziness, which should instead be positive. Page 149 currently indicates migraine frequency during the past 12 months as “weekly”, which should be “daily”.
Page 150 asks for the effects on usual occupation and resulting work problem, to which Dr. Tuna responded: "difficulty concentrating at work when migraines occur". This is grossly understated, in my opinion, as is the response to "Are there effects of this problem on normal activities?” which is simply “No.” I must admit that I am simply stupefied as to how this is selected as the appropriate response when I am unable to make significant long term plans due to the unpredictability of my issues, am forced to spend many days simply waiting in the dark for the current attack to pass, and must currently be considered unemployable due to the sheer volume of time in which I would be unable to perform job related tasks. In point of fact, many short term trips (to the store and such) have had to be aborted due to rapid onset of symptoms without warning shortly after leaving the house. Quite apart from the “normal” level of discomfort and incapacitation that I have been experiencing up to this point, the severity of my symptoms has continued to accelerate, to the point that I was forced to seek care through the emergency department on 6/28/11 at Southwest Washington Hospital, as well as the Portland VA emergency department on 7/1/11, 8/18/11, 8/21/11, 8/22/11, and 9/08/11. I have also had increasing experiences with migraines lasting multiple days without break.
On page 151, Dr. Tuna states “The condition/disability headaches/migraines is not caused by or a result of service (and/or exposure to environmental toxins). Rationale for opinion given: No medical documentation of headaches/migraines in service (in fact veteran uniformly responded ‘no’ to headaches in all health questionnaires in service). No basis in medical fact to assert environmental toxin exposure resulted in headaches/migraines.” As indicated previously in this response, several records of medical visits documenting intervals of increased blood pressure and dizziness/tingling in the extremities during my service in Japan are missing, and my headaches at that time were within a range that were attributed to this increase in blood pressure, rather than being a symptom on their own. Insofar as these not being related to environmental toxins, I would refer you to enclosure #5, Page 23, and enclosure #9, page 3and 7, which outline headache/migraine associated with exposure. Enclosure #15 specifically indicates that among the toxins personnel were exposed to, carbon tetrachloride, cadmium, chloroform, mercury, trichlorethene, vinyl chloride, and 1,3-Dichloropropene are known to cause headache/migraine.
Also on page 151, Dr. Tuna states “The condition/disability pain due to light sensitivity (causing migraines) is not caused by or a result of service (or environmental toxin exposure). Rationale for opinion given: The only light sensitivity noted in the SMR’s was secondary to a single episode of acute conjunctivitis, which resolved. The conjunctivitis was likely the cause of both the ‘pain’ and ‘light sensitivity’ noted. No subsequent light sensitivity is documented, and none is associated with headaches or pain. There is no basis in medical fact to assert that environmental toxin exposures have resulted in pain due to light sensitivity.” I am not entirely sure as to why this is broken out as separate from my migraines, but my initial headaches were mild enough and infrequent enough that I did not experience or associate light sensitivity with my migraine symptoms until some years after my military service, nor was visual aura prominent enough to be identified as an ongoing symptom.
On page 152, Dr. Tuna states “The condition/disability chronic bloody discharge from the nose is not caused by or a result of service (including exposure to environmental toxins) Rationale for opinion given: Normal nose exam, no medical documentation of any bloody noses. The veteran repeatedly responded ‘no’ to medical questionnaires asking about any nose problems, while in service. There is no basis in medical fact to assert that toxin exposures have caused chronic bloody noses.” This is inaccurate; Pages 14, and 75-76 of my Navy medical record document the increased breathing difficulty and bloody nasal discharge I experienced during my time in Japan. Insofar as these not being related to environmental toxins, I would refer you to enclosure #3, Page 2, enclosure #5, Page 23-24, and enclosure #9, page 3 and 7, which outline breathing issues associated with exposure. Enclosure #15 specifically indicates that among the toxins personnel were exposed to, arsenic, beryllium, cadmium, nitrogen dioxide, particulate matter, sulfur dioxide, vinyl chloride, 1,2-Dichlorethane, 1,2-Dichloropropane, and 1,3-Dichloropropene are known to cause respiratory issues.
Also on page 152, Dr. Tuna states “The condition/disability psoriasis L pre-tibial area is at least as likely as not (50/50 probability) caused by or a result of service. Rationale for opinion given: SMR’s appear to support the diagnosis of psoriasis in the same area identified on exam today. The total amount of skin involvement appears stable or less than initially reported years ago.” This is only somewhat inaccurate, as the psoriasis initially appeared on the upper surface of my left foot and occupied an area approximately half the size of the current area. Pages 13, 23-25, and 75-76 of my Navy medical record document the skin irritation and psoriasis that developed during my enlistment. Insofar as this being related to environmental toxins, I would refer you to enclosure #3, page 7, enclosure #5, page 7 and 23, enclosure #8, page 2 and 12-13, and enclosure #9, page 3 and 7, which outline skin issues associated with exposure. Enclosure #15 specifically indicates that among the toxins personnel were exposed to, arsenic, cadmium, carbon tetrachloride, trichlorethelene, 1,2-Dichlorethane , 1,2-Dichloropropane, 1,3-Dichloropropene, and 2,3,7,8-tetrachlorodibenzo-paradioxin are known skin irritants. In addition to the symptoms specifically discussed in Dr. Tuna’s stated opinions, the nausea that was skipped over in the questionnaire is indicated as a known issue in enclosure #5, page 24, and enclosure #9, page 3 and 7, which outline nausea as one of the symptoms associated with exposure. Enclosure #15 specifically indicates that among the toxins personnel were exposed to, arsenic, cadmium, carbon tetrachloride, chloroform, mercury, trichlorethene, and 1,2-Dichlorethane are known to cause nausea. Also skipped over were symptoms of vomiting, which are specifically indicated in enclosure #15 as potentially caused by cadmium, carbon tetrachloride, trichlorethelene, and 1,2-Dichlorethane, among the chemical toxins personnel were exposed to.
Additional symptoms experienced during or associated with these migraine attacks but not mentioned by the questionnaire are chest pain/angina (mentioned as a potential effect in enclosure #9, page 3, and acknowledged as potentially caused by exposure to beryllium and mercury in enclosure #15), anosmia (acknowledged as potentially caused by exposure to camium in enclosure #15), depression (acknowledged as potentially caused by exposure to chloroform in enclosure #15), dizziness (acknowledged as potentially caused by exposure to carbon tetrachloride, chloroform, trichlorethelene, vinyl chloride, 1,2-Dichloropropane, and 1,3-Dichloropropene in enclosure #15), irritability (acknowledged as potentially caused by exposure to chloroform in enclosure #15), insomnia (acknowledged as potentially caused by exposure to lead and mercury in enclosure #15), along with memory, concentration, confusion, and attention issues (acknowledged as potentially caused by exposure to mercury and trichlorethelene in enclosure #15).
Finally, also on page 152, Dr. Tuna states "Due to the veteran being an unreliable historian, it would be mere speculation to comment on unemployability due to migraine headaches. These headaches do not appear to be service connected in any event." I would respond that I have been as faithful a historian as has been practical under the circumstances, and have given the VA access to all available medical records, given my infrequent medical coverage over the years. The catastrophic effect of these migraines on my employability should be self evident, and the connection of these migraines with my service in Japan should be considered to be well proven, as they are listed as a known effect in several of the attached enclosures, and the latency period of associated symptoms is well documented.
Thus far, my experience with the VA health system has been haphazard at best, with some physicians providing excellent, informed service, and others simply seeming content with barely going through the motions. An example would be the experience that I have recently had with the nurse practioner initially assigned as my primary care giver. While her support staff seemed both eager and adequate, over the six months that I was officially under her care, I spent a total of 45 minutes speaking with her, the bulk of which occurred during my intake interview. Calls for follow up care following ER visits and repeated requests for referral to specialist(s) and additional testing were simply ignored, finally culminating in a necessary request for reassignment to another provider. My current referral to a staff neurologist actually came through the emergency department, after having been berated again during my third visit of the week for not following up with more qualified personnel.
Currently, I am experiencing extremely painful migraines lasting 6-8 hours per session, usually twice per day, and often punctuated by vomiting triggered by the sheer level of pain experienced during intermittent spikes of severity. Secondary effects concurrent with these attacks include dizziness, nausea, confusion, aphasia, aura, visual distortion, light and sound sensitivity. I spend a significant amount of time simply lying in the dark, trying desperately to avoid any additional stimulus that might further aggravate my symptoms, compromising my ability to participate social or productive activities, much less employment. I have also recently begun experiencing periods of crushing chest pain/angina lasting between 5-90 minutes per attack, and have experienced over a dozen of these attacks over the past two months. I’ve had insomnia for years now due to the pain interfering with sleep patterns, and have intermittent night terrors, especially during periods where I pass out while still in pain.
Frankly, at this point I’m very concerned about my situation. I’m scared that the pace and severity of these issues will continue to accelerate, and that further issues associated with my time in Atsugi will continue to surface. The extreme latency of known issues means that I will not likely know all of the long term effects for decades to come. I’m concerned for my fellow service members, who may not be aware of the health issues that have been incurred by their service alongside me in Japan. If it were not for the current severity of my own issues, I myself would not have known of the connections between the smog that bathed our housing units daily and the illnesses I have now, nor would I have known that I was entitled to care through the VA, as I found out last year.
At the time, the command made almost no effort to disseminate information, and minimized any potential risk verbally, despite multiple investigations into health risks and ongoing complaints issued to both the Japanese government and the Shinkampo operators. The sum total of guidance offered to me and my wife was a single 2 page flyer (Enclosure #3) outlining minor short term respiratory issues and a nearly infinitesimal potential increase in cancer rates for a very long length of exposure. We certainly weren’t made aware of the 240+ toxins found during these investigations, nor the additional known diseases and effects likely to be caused by exposure to these. In addition, neither myself nor any of these shipmates that I maintain contact with were contacted about these issues after our period of service in Japan, despite a directive to establish a registry of affected service members.
Further, I’m concerned about the long term effects of this on my mental status. My first wife, Jessie, had numerous health issues during her stay on base, including migraine, bronchitis, depression, and endometriosis, all of which only worsened as her time on Atsugi lengthened. She was driven to attempt suicide twice, and finally passed away in early 2001. I find myself scared that my own path will eventually follow hers, and that I will lose control of my faculties. The progress of my issues has gotten bad enough that my family have become scared of my actions during an attack, and my wife has asked that I carry her information on a prominent and easily accessible card so that she may be contacted if I am incapacitated.
In conclusion, I would invite the VA to examine the enclosed documentation, much of which was generated by the Atsugi command or under direction from the command. If more in depth C&P examinations are required, I will willingly make myself available for the appropriate testing, but would hope that the experience of having my responses to questions about my medical history simply being assumed to be negative without actually being asked would not be repeated. Thank you for your time,
Sincerely,
Josh *******
I hereby certify that the information I have given is true to the best of my knowledge and belief.
Signed 9/20/11 _______________________
Enclosures: Enclosure #1, Navy Medical Record, Joshua A. Byram, 1995-2000, 80 pages [Purpose of inclusion: To provide a complete record of my navy medical history, as given to me]
Enclosure #2, VA Medical Record, Joshua A. Byram, March 7, 2011-September 14, 2011, 200 pages [Purpose of inclusion: To provide a complete record of my VA medical history since joining the VA system on March 7, 2011]
Enclosure #3, Health and Environmental Fact Sheet #1, 3 pages (retrieved from: http://www-nehc.med.navy.mil/downloads/ep/Atsugi/FACTSHT1.pdf) [Purpose of inclusion: To illustrate the sum total of health information offered to myself and my wife upon being moved to on base housing]
Enclosure #4, Compensation and Pension Service Bulletin – October 2009, 8 pages (Excerpt, pages 1-2, retrieved from: http://www.atsugi-incinerator-group.com/CP_Bulletin_Oct_09.pdf?attredirects=0) [Purpose of inclusion: To direct Compensation and Pension personnel to their own internal guidance on this issue]
Enclosure #5 - US DOJ Petition from RADM Haskins on 22Aug97 to Governor Kanagawa.pdf, 28 pages (retrieved from: http://sites.google.com/site/srpusmc/USDOJPetition22Aug97GovernorKanagawa.pdf?attredirects=0) [Purpose of inclusion: To confirm that the USN was aware of environmental hazards at the highest levels, to confirm toxins found within incinerator output, and to confirm known health issues associated with same]
Enclosure #6, U.S. Senate Committee Letter and response from DOD & VA, 9 pages (retrieved from: http://www.atsugi-incinerator-group.com/SOCenvirotoxins09.pdf?attredirects=0) [Purpose of inclusion: Guidance for confirmation of exposure locations and times]
Enclosure #7, VA/DOD Response to Certain Military Exposures, 166 pages (Excerpt, pages 10, 21, 49-62, 76-82, 103, 118-123, 132-134, retrieved from: http://veterans.senate.gov/upload/10_08_09.rtf) [Purpose of inclusion: To provide official dialogue and responses regarding this issue, illustrate the effects on other residents and the extremely limited response by base authorities in controlling exposure]
Enclosure #8 - 2009 NAF Atsugi Health Study, NMCPHC, Executive Summary, 17 pages (retrieved from: http://www.atsugi-incinerator-group.com/NMCPHCJuly09ExecutiveSummaryNAFAtsug.pdf?attredirects=0) [Purpose of inclusion: To illustrate effects of exposure as indicated by the health study, to confirm a number of the known toxins that residents were exposed to, to indicate the inherent limitations assumed by these studies due to non-inclusion and issue latencies]
Enclosure #9, 97 Medical Effects and Pregnancy Study, 8 pages (retrieved from: http://www.atsugi-incinerator-group.com/97MedicalEffectsandPregnancyStudy.pdf?attredirects=0) [Purpose of inclusion: To provide study results for service members still working on base at the time of study as opposed to latent effects, to provide an alternate sampling of known toxins that residents were exposed to]
Enclosure #10, 98 Human Health Risk Assessment Atsugi, 47 pages (Excerpt, pages 14-15, 32-33 retrieved from: target="_blank">http://www.atsugi-incinerator-group.com/98HumanHealthRiskAssessmentAtsugi.pdf?attredirects=0) [Purpose of inclusion: To provide information as to concentrations of known pollutants provided by the incinerator]
Enclosure #11, EPA Mini-case studies, 29 pages (Excerpt, pages 3-5, retrieved from: http://epa.gov/osp/regions/minicase.pdf) [Purpose of inclusion: To illustrate pollutant concentration as derived from soil sampling at various distances from the incinerator]
Enclosure #12, Skywriter, October 10, 1997, Page 2, Captain’s Call, 1 page (retrieved from: http://sites.google.com/site/nafatsugi2/97CaptianCallNotransfers.pdf?attredirects=0) [Purpose of inclusion: To illustrate lack of concern from leadership as well as lack of information dissemination as to the seriousness of health concerns]
Enclosure #13, Email from u00pa2b@cpf.navy.mi on 8-7-98, 2 pages (retrieved from: http://sites.google.com/site/nafatsugi2/97EmaildataPeoplearenotawareonarriva.pdf?attredirects=0) [Purpose of inclusion: To illustrate that, at some level, command personnel were well aware of the seriousness of the situation and that there was a wide disconnect between that level and the level of concern conveyed as appropriate to base personnel]
Enclosure #14, Text of S.3378 as Placed on Calendar Senate, 4 pages (retrieved from: http://www.opencongress.org/bill/111-s3378/show) [Purpose of inclusion: To illustrate senate concern and action with regard to former NAF Atsugi personnel]
Enclosure #15 - Toxin Chemicals that exceeded EPA standards at NAF Atsugi, Japan, 16 pages (retrieved from: http://www.atsugi-incinerator-group.com/health) [Purpose of inclusion: To illustrate known connections between exposed toxins and associated health effects]
The short version of their findings is: "You don't have any significant issues, and even if you did, we didn't do it." Wrong answer, buddy. The examinations in question were completely screwed up, and in several cases, the examiner simply assumed information that was completely incorrect, in effect falsifying information to provide answers that were more favorable to their side of the table. Seriously not good juju, there.
So, basically, I've been spending the last couple of days working with my local rep and putting together an appropriately scathing and articulate response, and gathering evidence that my issues have been acknowledged as probable effects of the toxin exposure I received in Japan, including some fun internal direction to the C&P department specifically on this subject. If you'd like a better idea of exactly what's going on, I've included the full text of my latest statement below, along with links to the evidence I'm submitting.
Also, as a special "treat" of sorts, I happened across a couple of videos that someone shot of the residential complexes on Atsugi while the incinerator was still in operation. Here they are, if you're curious as to what Jessie and I were living in for a couple of years, especially during the half of the year that winds directed the smog directly to us.
The good news is that my new nurse practicioner seems to be significantly better than my last one, and I've got a number of tests scheduled over the next few months that might help me lock down what's actually wrong a little better.
Joshua ********** – Reference – ********** – File # ********** - Statement in Support of Claim 2
(As dictated to, edited, and organized by Eden **********) September 19, 2011
As my ongoing symptoms of migraine and associated secondary effects have continued to worsen over the past several months, I recently requested a copy of my VA medical health record since March of this year, so that I might provide these reports as additional supporting evidence for my disability claim. Among the reports provided were copies of my Compensation and Pension benefit exams, and I must say that I was dismayed, insulted, and incensed by the opinions given, as well as the manner in which these examinations were given (rushed, incomplete, and in some cases, information/answers assumed by the examiner without bothering to ask relevant questions). Further, I wish to take this opportunity to respond to those opinions and to provide further evidence as appropriate prior to the VA rendering an initial decision on my case, so as to avoid the delay and expense that might be incurred by necessitating an appeal to that decision if it were to be based on these opinions alone.
Firstly, I would like to address a number of discrepancies and note a few items in the two records provided to me. Enclosure #1 is my Navy Medical Record, as provided to me upon discharge. I’d like to note that my separation physical was provided by a pharmacy assistant (as noted on Page 12, 23Oct00), rather than an actual physician, and thus may be considered somewhat suspect in thoroughness. When I left Japan (as noted on page 14, 18Jan00), more frequent colds, sinus congestion, and a pattern of progressively decreasing health were documented already, although my symptoms hadn’t increased to the debilitating level that they have assumed in recent years. Pages 15-19 document that I had been given Health and Environmental Fact Sheet, NAF Atsugi #1 (included as Enclosure #3) as part of the move to on base housing with my first wife, Jessie. I should point out that this move was not optional, and was in fact required as soon as space in on base housing opened up – at no point was an alternative to on base housing made available to service members expressing concern over these environmental issues, and the potential effect of those issues was verbally minimized in every possible way by housing personnel. Additionally, my wife and I were located in building 3056, just over 500 meters from the incinerators in question, and thus had very high exposure to the pollutants throughout our time there.
Pages 10, 13, and 22 document the decrease in hearing acuity that I suffered over my term of service. Pages 13, 23-25, and 75-76 document the skin irritation and psoriasis that developed during this time. Pages 14. and 75-76 document the increased breathing difficulty and bloody nasal discharge over the same period. Conspicuously missing are records of the half dozen or so visits to the doctor that I had documenting intervals of increased blood pressure and dizziness/tingling in the extremities during my service in Japan (the headaches that I currently suffer had not increased to catastrophic level at this time, and thus were attributed to this blood pressure increase). I would like to request that copies of my original medical records from NAF Atsugi and CTF 72 Kami Seya be obtained to provide records of these incidents.
Enclosure #2 is my VA Medical Record, as printed electronically on September 14th, 2011. Pages 44 and 49 both list my habits as drinking rarely; in point of fact I have not drunk alcohol since April of this year, at which point I was asked to discontinue my already infrequent alcohol use so as to avoid additional stress on my system. Pages 24, 64, 67, 70, 73, 76, 79, 83, 86, 88, 91, 94, 97, and 101 all indicate that Topirimate is in current use at the time of respective examinations; this was discontinued on 8/01/11. Page 26 indicates that my mother has dementia and that I had lost 10 lbs; it is my maternal grandmother that had dementia, and I had lost 23 lbs at that point. Page 130 lists ADHD as being symptomatic since childhood; this is incorrect – in fact symptoms have only been present since my military service, and I was not diagnosed as having ADHD until 2006 by Dr. Julien ********** of the Corvallis Clinic in Oregon.
Pages 104-111 are the findings of Dr. Dillon on 8/15/11 for my mental health evaluation for compensation and pension. I disagree with his findings on several specific points. I do, in fact, agree with at least part of his statement on page 105, "...Mr. Byram's depression (including memory gaps) is more likely than not caused by his headaches.", and will in fact state unequivocally that my current depression revolves entirely around my migraines and associated symptoms; I would regard my depression as a secondary symptom of same. As to my memory issues, it is unclear to me how much of that issue is directly related to the headaches and how much is a tertiary symptom created by said depression, or if in fact this is an unrelated symptom created through my toxin exposure at Atsugi.
On page 107, Dr. Dillon selected the response: "Occupational and social impairment with occasional decrease in work efficiency and intermittent periods of inability to perform occupational tasks, although generally functioning satisfactorily, with normal routine, self-care, and conversation." – I would more accurately characterize my situation with this response, found on the same page: "Occupational and social impairment with deficiencies in most areas, such as work, school, family relations, judgment, thinking, and/or mood." He also states that "The veteran's occupational and social impairment is due to his psychological distress/depression." – I disagree with this wholeheartedly. My difficulties with school, work, and social life revolve entirely around my migraines, the inactive time required by them, the difficulty in thinking during an attack, lack of concentration and distraction provided by the severity of the pain and secondary effects, as well as the unpredictability of their pattern. Currently, my symptoms have increased to the point that I have migraines lasting 8-12 hours daily, incurring extreme pain, nausea, dizziness, and provide extreme sensitivity to light and sound as well as visual and spatial distortion. Friends and family have noted an increase in my general irritability, a decrease in logical thinking, and a general depressive mood, typified in the most extreme cases by some level of suicidal ideation during the most severe periods. Onset of symptoms has become both rapid and erratic, causing me to have to forgo driving for myself if at all possible since June of this year.
When I was laid off in 2009, part of the reason that I chose not to return to the workforce and instead attempt to change career fields by going back to school was as a delaying strategy to decrease the level of activity required of me from day to day in response to the increasing severity of my symptoms at that time. I had hoped to find some combination of medicine and/or avoidance of triggering effects that might allow me to decrease the impact of these issues. Instead, symptoms have only worsened since that point, eventually leading to a decision to withdraw from school in June of this year. Eventually, I came to the realization that further time at school at this level of medical control would only serve to increase my debt in terms of school loans without providing significant educational benefit.
On page 109, Dr. Dillon typifies my memory issues as: "Mild memory loss, such as forgetting names, directions, or recent events" – I would argue that the selection of "Impairment of short and long term memory, for example, retention of only highly learned material, forgetting to complete tasks", found on the same page, would be more accurate. At this point, nearly all of my memories of times before the last year or so is missing, and is only able to be mildly prompted by photos and letters from those years. The three years that I had with my first wife, Jessie, are almost entirely gone, and in point of fact, I have great difficulty in even being able to call her to mind. More recent events are, at best, blurry and indistinct, retaining only the most general outlines of experience. Insofar as short term memory is concerned, my daily life has become almost entirely dependent upon electronic alarms and aids, such as writing notes to myself for nearly any issue or concern via my mobile phone, as well as prompting by those around me.
Pages 133-153 are the findings of Dr. Tuna on 6/30/11 for my physical health evaluation for compensation and pension. While I do disagree with several of his findings, and will speak to this further later, the most concerning and immediate issue that I would like to address is that several sections of questions were skipped outright during the interview and simply marked as negative. I would like to address those here. On page 136-138, the sections “Genitourinary ROS” and “Abdominal/Gastrointestinal ROS” were skipped entirely and marked negative.
For Genitourinary ROS, I was not asked if there was a history of abnormal flow, urgency, dysuria, hesitancy, testicular pain, scrotal mass, erectile dysfunction, genital lesions, urethral discharge, flank pain, hematuria, stones, urinary frequency, nocturia, urinary incontinence, dialysis, obstructive voiding, repetitive urinary infection. Accordingly, hesitancy and erectile dysfunction are currently marked as negative and should instead be positive.
For Abdominal/gastrointestinal ROS, I was not asked if there was a history of nausea, vomiting, diarrhea, constipation, indigestion, heartburn, hemmoroids, hernia, abdominal mass, abdominal swelling, regurgitation, jaundice, fecal incontinence, post-prandial symptoms, dysphagia, hematemesis, melena, pancreatitis, gallbladder attacks, abdominal pain. Accordingly, nausea, vomiting, heartburn, gallbladder attacks, and abdominal pain are all currently marked as negative and should instead be positive.
On page 138, under Psychiatric ROS, history of speech difficulty, memory problems, and sleep impairment are all currently marked negative and should be positive. I often experience aphasia during migraine attacks, have extensive memory issues as indicated above, and currently experience both insomnia and night terrors. Both page 144 and 147 indicate that I was currently in school at the time of examination, when in fact I had already stopped going to school. Page 145 indicates no history of dizziness, which should instead be positive. Page 149 currently indicates migraine frequency during the past 12 months as “weekly”, which should be “daily”.
Page 150 asks for the effects on usual occupation and resulting work problem, to which Dr. Tuna responded: "difficulty concentrating at work when migraines occur". This is grossly understated, in my opinion, as is the response to "Are there effects of this problem on normal activities?” which is simply “No.” I must admit that I am simply stupefied as to how this is selected as the appropriate response when I am unable to make significant long term plans due to the unpredictability of my issues, am forced to spend many days simply waiting in the dark for the current attack to pass, and must currently be considered unemployable due to the sheer volume of time in which I would be unable to perform job related tasks. In point of fact, many short term trips (to the store and such) have had to be aborted due to rapid onset of symptoms without warning shortly after leaving the house. Quite apart from the “normal” level of discomfort and incapacitation that I have been experiencing up to this point, the severity of my symptoms has continued to accelerate, to the point that I was forced to seek care through the emergency department on 6/28/11 at Southwest Washington Hospital, as well as the Portland VA emergency department on 7/1/11, 8/18/11, 8/21/11, 8/22/11, and 9/08/11. I have also had increasing experiences with migraines lasting multiple days without break.
On page 151, Dr. Tuna states “The condition/disability headaches/migraines is not caused by or a result of service (and/or exposure to environmental toxins). Rationale for opinion given: No medical documentation of headaches/migraines in service (in fact veteran uniformly responded ‘no’ to headaches in all health questionnaires in service). No basis in medical fact to assert environmental toxin exposure resulted in headaches/migraines.” As indicated previously in this response, several records of medical visits documenting intervals of increased blood pressure and dizziness/tingling in the extremities during my service in Japan are missing, and my headaches at that time were within a range that were attributed to this increase in blood pressure, rather than being a symptom on their own. Insofar as these not being related to environmental toxins, I would refer you to enclosure #5, Page 23, and enclosure #9, page 3and 7, which outline headache/migraine associated with exposure. Enclosure #15 specifically indicates that among the toxins personnel were exposed to, carbon tetrachloride, cadmium, chloroform, mercury, trichlorethene, vinyl chloride, and 1,3-Dichloropropene are known to cause headache/migraine.
Also on page 151, Dr. Tuna states “The condition/disability pain due to light sensitivity (causing migraines) is not caused by or a result of service (or environmental toxin exposure). Rationale for opinion given: The only light sensitivity noted in the SMR’s was secondary to a single episode of acute conjunctivitis, which resolved. The conjunctivitis was likely the cause of both the ‘pain’ and ‘light sensitivity’ noted. No subsequent light sensitivity is documented, and none is associated with headaches or pain. There is no basis in medical fact to assert that environmental toxin exposures have resulted in pain due to light sensitivity.” I am not entirely sure as to why this is broken out as separate from my migraines, but my initial headaches were mild enough and infrequent enough that I did not experience or associate light sensitivity with my migraine symptoms until some years after my military service, nor was visual aura prominent enough to be identified as an ongoing symptom.
On page 152, Dr. Tuna states “The condition/disability chronic bloody discharge from the nose is not caused by or a result of service (including exposure to environmental toxins) Rationale for opinion given: Normal nose exam, no medical documentation of any bloody noses. The veteran repeatedly responded ‘no’ to medical questionnaires asking about any nose problems, while in service. There is no basis in medical fact to assert that toxin exposures have caused chronic bloody noses.” This is inaccurate; Pages 14, and 75-76 of my Navy medical record document the increased breathing difficulty and bloody nasal discharge I experienced during my time in Japan. Insofar as these not being related to environmental toxins, I would refer you to enclosure #3, Page 2, enclosure #5, Page 23-24, and enclosure #9, page 3 and 7, which outline breathing issues associated with exposure. Enclosure #15 specifically indicates that among the toxins personnel were exposed to, arsenic, beryllium, cadmium, nitrogen dioxide, particulate matter, sulfur dioxide, vinyl chloride, 1,2-Dichlorethane, 1,2-Dichloropropane, and 1,3-Dichloropropene are known to cause respiratory issues.
Also on page 152, Dr. Tuna states “The condition/disability psoriasis L pre-tibial area is at least as likely as not (50/50 probability) caused by or a result of service. Rationale for opinion given: SMR’s appear to support the diagnosis of psoriasis in the same area identified on exam today. The total amount of skin involvement appears stable or less than initially reported years ago.” This is only somewhat inaccurate, as the psoriasis initially appeared on the upper surface of my left foot and occupied an area approximately half the size of the current area. Pages 13, 23-25, and 75-76 of my Navy medical record document the skin irritation and psoriasis that developed during my enlistment. Insofar as this being related to environmental toxins, I would refer you to enclosure #3, page 7, enclosure #5, page 7 and 23, enclosure #8, page 2 and 12-13, and enclosure #9, page 3 and 7, which outline skin issues associated with exposure. Enclosure #15 specifically indicates that among the toxins personnel were exposed to, arsenic, cadmium, carbon tetrachloride, trichlorethelene, 1,2-Dichlorethane , 1,2-Dichloropropane, 1,3-Dichloropropene, and 2,3,7,8-tetrachlorodibenzo-paradioxin are known skin irritants. In addition to the symptoms specifically discussed in Dr. Tuna’s stated opinions, the nausea that was skipped over in the questionnaire is indicated as a known issue in enclosure #5, page 24, and enclosure #9, page 3 and 7, which outline nausea as one of the symptoms associated with exposure. Enclosure #15 specifically indicates that among the toxins personnel were exposed to, arsenic, cadmium, carbon tetrachloride, chloroform, mercury, trichlorethene, and 1,2-Dichlorethane are known to cause nausea. Also skipped over were symptoms of vomiting, which are specifically indicated in enclosure #15 as potentially caused by cadmium, carbon tetrachloride, trichlorethelene, and 1,2-Dichlorethane, among the chemical toxins personnel were exposed to.
Additional symptoms experienced during or associated with these migraine attacks but not mentioned by the questionnaire are chest pain/angina (mentioned as a potential effect in enclosure #9, page 3, and acknowledged as potentially caused by exposure to beryllium and mercury in enclosure #15), anosmia (acknowledged as potentially caused by exposure to camium in enclosure #15), depression (acknowledged as potentially caused by exposure to chloroform in enclosure #15), dizziness (acknowledged as potentially caused by exposure to carbon tetrachloride, chloroform, trichlorethelene, vinyl chloride, 1,2-Dichloropropane, and 1,3-Dichloropropene in enclosure #15), irritability (acknowledged as potentially caused by exposure to chloroform in enclosure #15), insomnia (acknowledged as potentially caused by exposure to lead and mercury in enclosure #15), along with memory, concentration, confusion, and attention issues (acknowledged as potentially caused by exposure to mercury and trichlorethelene in enclosure #15).
Finally, also on page 152, Dr. Tuna states "Due to the veteran being an unreliable historian, it would be mere speculation to comment on unemployability due to migraine headaches. These headaches do not appear to be service connected in any event." I would respond that I have been as faithful a historian as has been practical under the circumstances, and have given the VA access to all available medical records, given my infrequent medical coverage over the years. The catastrophic effect of these migraines on my employability should be self evident, and the connection of these migraines with my service in Japan should be considered to be well proven, as they are listed as a known effect in several of the attached enclosures, and the latency period of associated symptoms is well documented.
Thus far, my experience with the VA health system has been haphazard at best, with some physicians providing excellent, informed service, and others simply seeming content with barely going through the motions. An example would be the experience that I have recently had with the nurse practioner initially assigned as my primary care giver. While her support staff seemed both eager and adequate, over the six months that I was officially under her care, I spent a total of 45 minutes speaking with her, the bulk of which occurred during my intake interview. Calls for follow up care following ER visits and repeated requests for referral to specialist(s) and additional testing were simply ignored, finally culminating in a necessary request for reassignment to another provider. My current referral to a staff neurologist actually came through the emergency department, after having been berated again during my third visit of the week for not following up with more qualified personnel.
Currently, I am experiencing extremely painful migraines lasting 6-8 hours per session, usually twice per day, and often punctuated by vomiting triggered by the sheer level of pain experienced during intermittent spikes of severity. Secondary effects concurrent with these attacks include dizziness, nausea, confusion, aphasia, aura, visual distortion, light and sound sensitivity. I spend a significant amount of time simply lying in the dark, trying desperately to avoid any additional stimulus that might further aggravate my symptoms, compromising my ability to participate social or productive activities, much less employment. I have also recently begun experiencing periods of crushing chest pain/angina lasting between 5-90 minutes per attack, and have experienced over a dozen of these attacks over the past two months. I’ve had insomnia for years now due to the pain interfering with sleep patterns, and have intermittent night terrors, especially during periods where I pass out while still in pain.
Frankly, at this point I’m very concerned about my situation. I’m scared that the pace and severity of these issues will continue to accelerate, and that further issues associated with my time in Atsugi will continue to surface. The extreme latency of known issues means that I will not likely know all of the long term effects for decades to come. I’m concerned for my fellow service members, who may not be aware of the health issues that have been incurred by their service alongside me in Japan. If it were not for the current severity of my own issues, I myself would not have known of the connections between the smog that bathed our housing units daily and the illnesses I have now, nor would I have known that I was entitled to care through the VA, as I found out last year.
At the time, the command made almost no effort to disseminate information, and minimized any potential risk verbally, despite multiple investigations into health risks and ongoing complaints issued to both the Japanese government and the Shinkampo operators. The sum total of guidance offered to me and my wife was a single 2 page flyer (Enclosure #3) outlining minor short term respiratory issues and a nearly infinitesimal potential increase in cancer rates for a very long length of exposure. We certainly weren’t made aware of the 240+ toxins found during these investigations, nor the additional known diseases and effects likely to be caused by exposure to these. In addition, neither myself nor any of these shipmates that I maintain contact with were contacted about these issues after our period of service in Japan, despite a directive to establish a registry of affected service members.
Further, I’m concerned about the long term effects of this on my mental status. My first wife, Jessie, had numerous health issues during her stay on base, including migraine, bronchitis, depression, and endometriosis, all of which only worsened as her time on Atsugi lengthened. She was driven to attempt suicide twice, and finally passed away in early 2001. I find myself scared that my own path will eventually follow hers, and that I will lose control of my faculties. The progress of my issues has gotten bad enough that my family have become scared of my actions during an attack, and my wife has asked that I carry her information on a prominent and easily accessible card so that she may be contacted if I am incapacitated.
In conclusion, I would invite the VA to examine the enclosed documentation, much of which was generated by the Atsugi command or under direction from the command. If more in depth C&P examinations are required, I will willingly make myself available for the appropriate testing, but would hope that the experience of having my responses to questions about my medical history simply being assumed to be negative without actually being asked would not be repeated. Thank you for your time,
Sincerely,
Josh *******
I hereby certify that the information I have given is true to the best of my knowledge and belief.
Signed 9/20/11 _______________________
Enclosures: Enclosure #1, Navy Medical Record, Joshua A. Byram, 1995-2000, 80 pages [Purpose of inclusion: To provide a complete record of my navy medical history, as given to me]
Enclosure #2, VA Medical Record, Joshua A. Byram, March 7, 2011-September 14, 2011, 200 pages [Purpose of inclusion: To provide a complete record of my VA medical history since joining the VA system on March 7, 2011]
Enclosure #3, Health and Environmental Fact Sheet #1, 3 pages (retrieved from: http://www-nehc.med.navy.mil/downloads/ep/Atsugi/FACTSHT1.pdf) [Purpose of inclusion: To illustrate the sum total of health information offered to myself and my wife upon being moved to on base housing]
Enclosure #4, Compensation and Pension Service Bulletin – October 2009, 8 pages (Excerpt, pages 1-2, retrieved from: http://www.atsugi-incinerator-group.com/CP_Bulletin_Oct_09.pdf?attredirects=0) [Purpose of inclusion: To direct Compensation and Pension personnel to their own internal guidance on this issue]
Enclosure #5 - US DOJ Petition from RADM Haskins on 22Aug97 to Governor Kanagawa.pdf, 28 pages (retrieved from: http://sites.google.com/site/srpusmc/USDOJPetition22Aug97GovernorKanagawa.pdf?attredirects=0) [Purpose of inclusion: To confirm that the USN was aware of environmental hazards at the highest levels, to confirm toxins found within incinerator output, and to confirm known health issues associated with same]
Enclosure #6, U.S. Senate Committee Letter and response from DOD & VA, 9 pages (retrieved from: http://www.atsugi-incinerator-group.com/SOCenvirotoxins09.pdf?attredirects=0) [Purpose of inclusion: Guidance for confirmation of exposure locations and times]
Enclosure #7, VA/DOD Response to Certain Military Exposures, 166 pages (Excerpt, pages 10, 21, 49-62, 76-82, 103, 118-123, 132-134, retrieved from: http://veterans.senate.gov/upload/10_08_09.rtf) [Purpose of inclusion: To provide official dialogue and responses regarding this issue, illustrate the effects on other residents and the extremely limited response by base authorities in controlling exposure]
Enclosure #8 - 2009 NAF Atsugi Health Study, NMCPHC, Executive Summary, 17 pages (retrieved from: http://www.atsugi-incinerator-group.com/NMCPHCJuly09ExecutiveSummaryNAFAtsug.pdf?attredirects=0) [Purpose of inclusion: To illustrate effects of exposure as indicated by the health study, to confirm a number of the known toxins that residents were exposed to, to indicate the inherent limitations assumed by these studies due to non-inclusion and issue latencies]
Enclosure #9, 97 Medical Effects and Pregnancy Study, 8 pages (retrieved from: http://www.atsugi-incinerator-group.com/97MedicalEffectsandPregnancyStudy.pdf?attredirects=0) [Purpose of inclusion: To provide study results for service members still working on base at the time of study as opposed to latent effects, to provide an alternate sampling of known toxins that residents were exposed to]
Enclosure #10, 98 Human Health Risk Assessment Atsugi, 47 pages (Excerpt, pages 14-15, 32-33 retrieved from: target="_blank">http://www.atsugi-incinerator-group.com/98HumanHealthRiskAssessmentAtsugi.pdf?attredirects=0) [Purpose of inclusion: To provide information as to concentrations of known pollutants provided by the incinerator]
Enclosure #11, EPA Mini-case studies, 29 pages (Excerpt, pages 3-5, retrieved from: http://epa.gov/osp/regions/minicase.pdf) [Purpose of inclusion: To illustrate pollutant concentration as derived from soil sampling at various distances from the incinerator]
Enclosure #12, Skywriter, October 10, 1997, Page 2, Captain’s Call, 1 page (retrieved from: http://sites.google.com/site/nafatsugi2/97CaptianCallNotransfers.pdf?attredirects=0) [Purpose of inclusion: To illustrate lack of concern from leadership as well as lack of information dissemination as to the seriousness of health concerns]
Enclosure #13, Email from u00pa2b@cpf.navy.mi on 8-7-98, 2 pages (retrieved from: http://sites.google.com/site/nafatsugi2/97EmaildataPeoplearenotawareonarriva.pdf?attredirects=0) [Purpose of inclusion: To illustrate that, at some level, command personnel were well aware of the seriousness of the situation and that there was a wide disconnect between that level and the level of concern conveyed as appropriate to base personnel]
Enclosure #14, Text of S.3378 as Placed on Calendar Senate, 4 pages (retrieved from: http://www.opencongress.org/bill/111-s3378/show) [Purpose of inclusion: To illustrate senate concern and action with regard to former NAF Atsugi personnel]
Enclosure #15 - Toxin Chemicals that exceeded EPA standards at NAF Atsugi, Japan, 16 pages (retrieved from: http://www.atsugi-incinerator-group.com/health) [Purpose of inclusion: To illustrate known connections between exposed toxins and associated health effects]
Friday, September 9, 2011
Yesterday, or, a time when records were set, new friends were met, but no long term answers, yet...
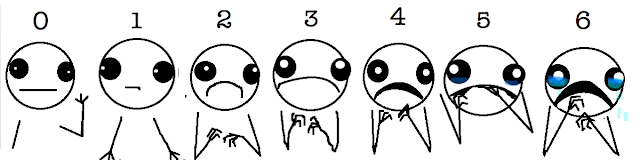

Eden actually pointed out a simply brilliant post from a webcomic called "Hyperbole and a half", recently, which highlights the plain inadequacy of the traditional pain scale used in doctor's offices these days. Unfortunately, I had entirely too much of a valid reason to use the proposed new scale, yesterday.
As it turns out, my respite from pain was a lot briefer than I had been hoping as of last post. Migraines, chest pain, and vomiting all made intermittent appearances over the last few days, culminating in the mother of all horrible experiences yesterday. I still don't know exactly what was going on, but I woke up in absolute agony shortly after midnight, with immense pressure and a sensation of fluid shifting around in my head - every change of angle for any reason whatsoever kicked the already nearly unbearable pain into extra high gear. Being absolutely exhausted, and frankly unable to face the thought of the movement involved in getting up and finding something to take the edge off the pain (not to mention not having the slightest idea what medication would be appropriate, as this felt so different from my normal modes), I spent the next few hours drifting between lying awake and getting just far enough into sleep to have absolutely terrifying dreams - somehow sleeping while in pain always seems to be about the only thing that produces dreams that I remember, and they're always just scary as hell; perhaps my normal sleep cycle just runs right past REM on the way to deep sleep in a desperate attempt to make up the many hours of sleep I tend to miss.
In any case, one of the dream cycles I landed in was just profoundly disturbing (this among dreams of being fired from working at Costco and being trapped in an underground apartment). For some reason, I ended up in a sequence that essentially had me convinced that my little brother, a man whom I've known, loved, and respected for approximately 28 years now, was a figment of my imagination. Now, I know that this sounds odd and unbelievable, but you have to understand, my normal memory is absolutely shattered at this point, most especially the memories from my childhood and early adulthood. Often, when my thoughts turn to my first wife, Jessie, for whatever reason, it's hard to feel that those years were real, given how little of our life together that I can recall. Kind of tragic, really, and not a fact that I care for, but I use it now as a comparison, because the dream had me feeling exactly the same way, that maybe the experiences I recalled with him were really all in my head. Regardless, I woke back up, still in horrible pain, and spent the better part of an hour and a half recounting the experiences I'd shared with him, and trying to convince myself that Tim actually existed. Perhaps this will give you some idea of how tenuous my hold on reality is at times, especially when I'm hurting for sleep.
The remainder of the night flowed by in much the same way, with dreams becoming less and less logical and pain continuing to get worse. I'm afraid that by the time Eden woke up, and eventually talked me into going in to the ER (I had myself quite convinced that they wouldn't be able to help me, that they would commit me for being suicidal, and that I wouldn't survive the trip to the ER due to the movement required), I had scared her quite a bit. Normally I'm a pretty stoic fellow, as I don't see the point of crying in most cases, and really don't have access to much emotion most of the time (left overs from the military and various traumatic periods, I think). This time, however, I managed to get myself into a hell of a state, somewhere between screaming and sobbing (Scrobbing?), as crying only made the pain that much worse, and of course, once started, it was awfully hard to calm down enough to stop. Surely unfairly scary to those around me, and I'm sorry for having exposed them to such a thing.
In the end, Eden did get me to the ER, with me holding on desperately to the seat and handle the whole way, trying valiantly to minimize movement from the most miniscule of bumps, with my eyes hidden behind both sunglasses and a wet washcloth. As I told the intake nurse, my pain was holding at a 10 ("the worst pain you've ever experienced" - prior to this point anyway) without movement, and was simply making up brand new numbers with any aggravating movement, crying, or the wondrously unpleasant experience of vomiting, which I'm afraid I had to dash away for twice while waiting for a bed to open up in the ER.
Of course they threw blood tests at me, and even took a CAT scan to be sure that there weren't any suspicious blobs showing up in my head to explain the nastiness, but in the end, they weren't able to come up with an explanation, other than possibly meningitis. Given that my temperature and other stats were in a normalish range, and that my pain was eventually managed, we decided to hold off on the spinal tap required to test for that against the symptoms returning in the next few days. Of course, to get my pain under control, they ended up piping in some Dilaudid, a morphine derivative that I hadn't been introduced to previously, along with a varied witches brew of anti-inflammatories and anti-histamines in my IV. Let me tell you, that's some pretty powerful stuff - quite unpleasant waves of sensation when first given, but insofar as A. covering pain, and B. making the remaining pain unimportant, that stuff is amazing. I went from pain quite literally off the scale to perhaps a 4 or a 5 in a matter of hours. Granted, I surely would have preferred some kind of answer for why things hurt so dang much, and I'm more than a little scared that it will return, but failing that, I'll take it. They even sent home two pills of it just in case, along with a few other meds, which I'm given to understand is quite unusual for that level of narcotic. The pain hasn't returned bad enough to make me resort to it yet, thankfully.
Actually, today hasn't been half bad - I woke up with very low static pain, but extremely high photophobia this morning, and so didn't accompany the girls to the swimming hole today, but even that faded for the most part in the afternoon after a dose of the anti-inflamitories and anti-histamines that the ER gave me to hold out until I can see my new doctor.
In point of fact, I don't have a new doctor - while the VA approved me leaving my previous nurse practitioner, they've simply assigned me to another one, as I mentioned last post. Oh well; I did get set up for an intake interview with her next Tuesday, so we'll see how that goes. I still do have some hope for the results of the MRI that my neurologist ordered - it should show much more soft tissue definition than the CAT scan, and thus may show different results. I have, however, given up on the elimination diet - it seems clear that dropping the major allergen possibilities from my diet had no significant impact over the week or so I was on it, although technically I suppose I could still have some environmental factors kicking in as allergens, so I'll still be asking for a test for that kind of thing.
So yes, that's where I'm at now - quite impressively horrible over the last few days, but at least today wasn't too bad at all. As Eden said, it's awfully nice to see me smile and laugh again (and it's awfully nice to have the attention span to do so - the fact that Ed Byrne is brilliantly funny helped too - we spent the evening watching some of his standup.)
Tuesday, September 6, 2011
Sitrep: So Far...
Well, I've got to admit to some confusion. It's Day 6 of my new elimination diet, and, as of yesterday, I was assuming that it wasn't bearing any fruit. The weekend was actually somewhat nice - horrible pain in the morning and evening, but I did get a few waking hours off in the afternoon to actually have some time to myself (pity it couldn't have been time that Eden was home). Yesterday was agonizing; woke up in pain at 3:30 am, and the darn thing didn't quit until 6pm - I was quite afraid that I'd bounced right into another multi-day cycle. All of this could easily be part of my normal variations in cycle; when I'm in the headache every day mode, it tends to shift by a bit off of a static 24 hour cycle, scrolling earlier or later at a whim, but generally somewhat stable.
Today, however, I woke up dizzy and nauseous, but with quite minimal pain. Still within the purview of my normal variation, but it seems to be tapering off somewhat, and I don't appear to be too very photophobic.
Long story short, I don't know where I'm at, but I guess there's something to be said for lack of negative confirmation. I'll be sticking to this diet (and lusting madly after soda and normal food - it probably doesn't help that I've been spending at least a little of my "useless" time reorganizing ebooks, and that I'm now in the cooking section) for another week or so, then will evaluate whether further investigation of allergy potentials is warranted.
Secondary thought: I did get a letter to the effect that I'm confirmed for being able to drop my useless nurse practitioner from the VA. The not so great news is that they've just switched me to a different NP. While I certainly have hope that the new one is going to be more useful and professional, part of the reason I had petitioned for the change was to get to an actual doctor; my understanding of the nurse practitioner program is that they are intended largely to handle the bulk of the "normal" cases; flus, upset stomachs, and the like, while freeing up the full MDs to handle the more esoteric cases, like mine. Ah well; it would be hard to have her be worse than the last.
The new Gabapentin hasn't arrived yet, so no news on how that's working. I'll keep you folks updated when I have more news.
Best wishes to all!
Today, however, I woke up dizzy and nauseous, but with quite minimal pain. Still within the purview of my normal variation, but it seems to be tapering off somewhat, and I don't appear to be too very photophobic.
Long story short, I don't know where I'm at, but I guess there's something to be said for lack of negative confirmation. I'll be sticking to this diet (and lusting madly after soda and normal food - it probably doesn't help that I've been spending at least a little of my "useless" time reorganizing ebooks, and that I'm now in the cooking section) for another week or so, then will evaluate whether further investigation of allergy potentials is warranted.
Secondary thought: I did get a letter to the effect that I'm confirmed for being able to drop my useless nurse practitioner from the VA. The not so great news is that they've just switched me to a different NP. While I certainly have hope that the new one is going to be more useful and professional, part of the reason I had petitioned for the change was to get to an actual doctor; my understanding of the nurse practitioner program is that they are intended largely to handle the bulk of the "normal" cases; flus, upset stomachs, and the like, while freeing up the full MDs to handle the more esoteric cases, like mine. Ah well; it would be hard to have her be worse than the last.
The new Gabapentin hasn't arrived yet, so no news on how that's working. I'll keep you folks updated when I have more news.
Best wishes to all!
Friday, September 2, 2011
Sitrep: Post-Neuro 1.0
For those that are waiting with bated breath for the outcome of my latest adventures in VA medicine, good news! Of sorts, anyway.
Turns out that the Neurologist I was assigned to, Dr. Daniel, appears to be both competent and compassionate. Long story short, he listened to what Eden and I had to say, gave comprehensive questions and answers, and seems pretty much at the top of his game. He's setting me up with a new maintenance med (preventative, rather than rescue) for migraine, Gabapentin, which is another anti-seizure med that's shown promise in migraine as well. I have a bit of trepidation about this, given how the last anti-seizure, Topirimate, went, but I at least have the strong feeling that he'll listen if things start going wrong again, and he has a backup med to try if this one is ineffective (an injectable form, but I don't recall the name off the top of my head).
In addition to this, we ran another bank of blood work yesterday, and I'm due to be set up for a full head MRI shortly to update my imaging (last was a CT scan in 2003-2004) and rule out a number of the nastier potential developments that might be causing all this, as well as mapping any possible occlusions or deformations of my sinuses, since I seem to be at least somewhet reactive to strong weather or pressure changes lately.
I'll have to follow up with him today, however, as Eden was doing her normal caretaker best to figure me out, and stumbled upon the current Wikipedia article on Cluster Headaches. Now, I've seen this term before, and it seemed to fit to some degree according to the definition that was available at the time (a very brief Mayo Clinic writeup), but there just wasn't a whole lot of information to flesh things out and I deadended on that line of research and moved on. This article, however, appears to fit my current symptoms (or at least my perception of them) to a "T", so I'm going to at least leave a voicemail to that effect for Dr. Daniel when it's a reasonable hour to see what he has to say and see if any change in our treatment plan is warranted with this specific fit.
I have to say, the colloquial nickname for this style of headache, the "suicide headache", is frighteningly apt. I must confess, it's an idea that has at least been circling the drain in my darkest hours during the last week-and-a-half long migraine, thanks in no small part to the incredibly miniscule sleep I was able to obtain for the duration. For what it's worth, this kind of thinking is WAY outside of my normal thought patterns, and was one of the neon warning signs that motivated me to get to the ER stat.
In any case, I'm chalking things up as having one more doctor on my side, and have high hopes that we'll be able to make significant progress in at least slowing or controlling my advancing symptoms. Bonus points: our food stamps finally came through from the state, so I'm also trying an elimination diet to try to rule out possible allergy triggers or agrivators. We'll see how that goes - most of yesterday was spent just being ravenous, despite Eden's wonderful salmon dinner. I'd attribute that largely to caffeine detox, personally, as well as the horrible brain-piercing night I've had. Regardless of said discomfort, it's a heck of a lot easier to take when it feels like I'm finally moving (or at least lurching) forward again.
Turns out that the Neurologist I was assigned to, Dr. Daniel, appears to be both competent and compassionate. Long story short, he listened to what Eden and I had to say, gave comprehensive questions and answers, and seems pretty much at the top of his game. He's setting me up with a new maintenance med (preventative, rather than rescue) for migraine, Gabapentin, which is another anti-seizure med that's shown promise in migraine as well. I have a bit of trepidation about this, given how the last anti-seizure, Topirimate, went, but I at least have the strong feeling that he'll listen if things start going wrong again, and he has a backup med to try if this one is ineffective (an injectable form, but I don't recall the name off the top of my head).
In addition to this, we ran another bank of blood work yesterday, and I'm due to be set up for a full head MRI shortly to update my imaging (last was a CT scan in 2003-2004) and rule out a number of the nastier potential developments that might be causing all this, as well as mapping any possible occlusions or deformations of my sinuses, since I seem to be at least somewhet reactive to strong weather or pressure changes lately.
I'll have to follow up with him today, however, as Eden was doing her normal caretaker best to figure me out, and stumbled upon the current Wikipedia article on Cluster Headaches. Now, I've seen this term before, and it seemed to fit to some degree according to the definition that was available at the time (a very brief Mayo Clinic writeup), but there just wasn't a whole lot of information to flesh things out and I deadended on that line of research and moved on. This article, however, appears to fit my current symptoms (or at least my perception of them) to a "T", so I'm going to at least leave a voicemail to that effect for Dr. Daniel when it's a reasonable hour to see what he has to say and see if any change in our treatment plan is warranted with this specific fit.
I have to say, the colloquial nickname for this style of headache, the "suicide headache", is frighteningly apt. I must confess, it's an idea that has at least been circling the drain in my darkest hours during the last week-and-a-half long migraine, thanks in no small part to the incredibly miniscule sleep I was able to obtain for the duration. For what it's worth, this kind of thinking is WAY outside of my normal thought patterns, and was one of the neon warning signs that motivated me to get to the ER stat.
In any case, I'm chalking things up as having one more doctor on my side, and have high hopes that we'll be able to make significant progress in at least slowing or controlling my advancing symptoms. Bonus points: our food stamps finally came through from the state, so I'm also trying an elimination diet to try to rule out possible allergy triggers or agrivators. We'll see how that goes - most of yesterday was spent just being ravenous, despite Eden's wonderful salmon dinner. I'd attribute that largely to caffeine detox, personally, as well as the horrible brain-piercing night I've had. Regardless of said discomfort, it's a heck of a lot easier to take when it feels like I'm finally moving (or at least lurching) forward again.
Subscribe to:
Posts (Atom)